


Highlights From The Comments On Semaglutide
...
Table of contents:
1. Top Comments
2. More Tips On Getting Cheap Semaglutide
3. Other Weight Loss Drugs
4. People Challenging My Numbers And Predictions
5. Do You Have To Stay On Semaglutide Forever Or Else Gain The Weight Back?
6. Personal Anecdotes
7. Tangents That I Find Tedious, But Other People Apparently Really Want To Debate
1. Top Comments
burritosol writes:
Great post! I’ve done some research on this issue, so here are a few thoughts. I put relevant links at the bottom of the post to support my specific claims.
First, the low volume for semaglutide that you are observing is at least partially due to supply shortages. The drug has been in serious shortage for a while. Novo Nordisk also sells Saxenda (liraglutide) for weight loss. Over the last 2 quarters, Saxenda sales are up 59%, while Wegovy sales are down 18%. Saxenda is priced similarly, and Wegovy is a better product. So I suspect a lot of the Saxenda spending would be going towards Wegovy in the absence of the semaglutide supply shortage.
Second, spending on Wegovy might not fully capture use of semaglutide for weight loss, because some people might be taking Ozempic primarily for weight loss benefits. Ozempic sales are huge, and it is a top-20 spending drug in Medicare. After the clinical trial was published showing sustained weight loss benefits from semaglutide, Ozempic sales growth accelerated (though sales were already growing fast). Even though Ozempic is approved for the diabetes indication, it makes sense that people would take it for weight loss, because (1) there is a big overlap between the obese and diabetic population and (2) Ozempic is more likely to be covered by insurance.
Third, your estimates of the costs are somewhat exaggerated, because the drug manufacturer pays significant discounts to insurers. These discounts do not reduce cost-sharing, but they do reduce premiums. When thinking about the social cost of the drug, it's more accurate to think about the price net of discounts, as opposed to the list price. The Morgan Stanley report that you cited reports roughly a 30% typical discount from the list price.
Fourth, this is nitpicky, but when you say "almost 10% of all US drug spending," you are dividing a 2030 spending projection by what U.S. prescription drug spending was in ~2020. The Medicare actuaries project U.S. prescription drug spending in 2030 to be closer to 600 million, not 300 million. That's still a massive projection for spending in the obesity class. If you believe the Morgan Stanley projection, spending on the obesity class as a share of national health spending will be comparable to peak spending on the Hepatitis C drugs. The financial impact of the Hepatitis C drugs was a huge story. But this would be even bigger, because the Hepatitis C drugs were a cure, such that the spending surge was short-lived. Conversely, the obesity drugs are chronic medications, and we should probably expect volume to continue to increase post-2030.
Fifth, a remarkable thing about semaglutide that may have been under-emphasized in your post is the extent to which the weight loss benefits are being sustained. People who successfully lose weight tend to have a very difficult time keeping the weight off. To my knowledge, before semaglutide, the only intervention that had been demonstrated to sustain a >10% weight loss benefit for more than 1-year was bariatric surgery. So far, clinical trails are showing sustained weight loss benefits from semaglutide for at least 2-years.
Sixth, this post focuses on GLP-1 agonists, which makes sense, because those drugs are starting to have an impact today. But the Morgan Stanley report also notes that amylin analogue cagrilintide may be approved for weight loss as soon as 2025. This drug has a completely different mechanism than semaglutide, but likely offers similar weight loss benefits. The crazy thing is that the weight loss benefits stack. So Novo Nordisk hopes to sell Cagrisema, which combines amylin analogue cagrilintide with semaglutide, and hopes to offer a ~30% average weight loss. This is roughly double what semaglutide offers, and is getting closer to bariatric surgery efficacy.
Seventh, if Medicare decides to cover Wegovy, it would be relatively affordable for Medicare beneficiaries. Starting in 2025, out-of-pocket costs for prescription drugs will be capped at $2,000 for Medicare beneficiaries. And most Medicare enrollees with a 30+ BMI are probably already spending a lot on drugs. So at the end of the day, the marginal cost might be $100 per month or even less. And if you are near-poverty, you get cost-sharing subsidies, so the cost is only about $10 per month. Of course, this all depends on Congress changing the law such that Medicare can cover obesity drugs. Currently, there is a statutory exclusion that can only be changed through Congressional action.
Thanks! I accept all the corrections as valid, and am as usual slightly miffed that my commenters know more than I do.
I most want to highlight the paragraph on the potential upcoming cagrilintide-semaglutide combination. Lots of commenters asked “okay, losing 15% body weight sounds good, but what if you need to lose more?” Probably the answer is “wait a few years for Cagrisema”.
Benjamin Jolley (blog) writes:
Compounding pharmacist here:
1) I’m not certain where other folks are getting semaglutide, but I would imagine Chinese pharma companies. You may have heard of the pharmacy in SLC, UT that attempted to compound hcq for COVID and sell it to the state of Utah? He bought it from a Chinese pharma company and what he eventually got busted for was false shipping manifests, not the blatant violation of the FDCA. I imagine something similar happened here.
2) while I can’t speak to the legality of sourcing the active ingredient, preparing the compound is probably legally fine. Wegovy and Ozempic has been in a shortage state for nearly 2 years now. In cases of shortages, I CAN legally compound products, including those protected by a patent or otherwise theoretically available. Patient access comes first- if I can’t source a finished product due to the manufacturer not having adequate supply, I’m good. I have to maintain documentation of my inability to source the patented products or the otherwise available product, but this is accepted practice. See, for example, this week’s FDA GFI re: compounding amoxicillin suspension for kids.
3) wegovy is sold in monthly dose paks, not weekly doses.
4) no, we don’t compound semaglutide in my pharmacy, and no I don’t intend to. The legal risks of compounding sterile products (ie injectables like this one) are intense enough for me to not do sterile products, let alone involving possible patent claims.
5) the savings card thing is “if your insurance pays something, we’ll cover most of your copay.” In the case of wegovy, they’ll pay up to $200/28 days for commercially insured prescriptions and up to $500/28 days for prescriptions paid out of pocket. The basis of these programs is that there is solid evidence that when prescriptions are >$50/month, people pick them up way less frequently. Coupons like these ShOULD be illegal, imo, as they basically invalidate the whole concept of copays and therefore allow pharma companies to Jack their prices into the stratosphere because the end user has no concept of the actual price. Without these cards, they would lower their prices so that people’s copays would typically hit a price of ~$50/month or less, out of pure profit maximization. (There’s also the fact that pharma pays rebates to PBMs to lower their prices are NOT used by those PBMs/insurers to set patient copays lower, ever, which is manifestly unfair and results in situations where people pay more for their insulin than their insurer has landed on with their rebates- ie the insurer collects a rebate so large that the patient is effectively subsidizing their insurer, rather than the other way around- I call this “reverse insurance”).
2. More Tips On Getting Cheap Semaglutide
Jason writes:
Practical update. I recently found that some varieties of Blue Cross Blue Shield insurance (through the federal employee program, at least) will now cover Wegovy (Ozempic) for weight loss, starting in January 2023. https://www.fepblue.org/open-season/whats-new-2023
Wegovy is on their formulary as a Tier 2 drug, meaning a copay of roughly $60/month. https://www.caremark.com/portal/asset/z6500_drug_list807_OE.pdf . I don’t know how common this will be in the coming year, but it’s a start.
Re canada, if you are american and have a prescription you should be able to get semaglutides for a couple hundred dollars a month through CanShipMeds. (At least, you could as of a couple months ago).
Sorry, I’m still not understanding this. Usualy weight loss dose of Wegovy is 2.4 mg per week = ~10 mg per month. The best I can find on CanShipMeds is 1 mg pens for $300. Doesn’t that suggest you’d need ten of those = $3000 per month? Or am I misunderstanding and that’s supposed to be the price for a month’s worth of 1 mg pens?
[update: Chad says this works with the oral form, still trying to learn more]
Mel on Calibrate, a group that offers semaglutide cheap ($25/month copay with most insurances):
IIRC Calibrate's pitch to insurers is that by pairing Semaglutide with their behaviour change program (app + coaches) they can eventually wean people off the medication while maintaining the weight loss effects, saving insurers lots of $$ in the long term. So far they've been quite successful convincing insurers (and VCs) of this but I think the evidence shows people need to stay on Semaglutide forever to maintain their weight so I don't think this will hold up.
I would be surprised if Semaglutide was cheaply available as a generic by the mid-2030s unless there are significant reforms made to the patent system or pharma industry rules. Humira and Lantus are good examples of drugs which would be significantly cheaper by now except for repeated patent extension and industry deals maintaining monopolies (although hopefully coming down soon).
Adam writes:
For what it's worth, Scott, though people may feel it isn't worth the risk due to not exactly being legal, it is fairly trivial to get semaglutide from a grey market lab that just buys bulk chemicals from Chinese raw suppliers to package and resell in western countries. At the one supplier I know for sure is selling tested, real stuff I've seen other people use and get results from, it's currently $120 for a two-month supply. But many, if not most, sellers of research peptides will stock this. You can even get reasonably-priced HGH if you want a little extra lipolysis kick, and in spite of the scare stories from moralizing legislators trying to make examples of pro athletes for cheating, it is extremely safe if you're not doing bodybuilder-level doses. Yet another thing anyone over the age of 40 can get a prescription for by going to any anti-aging clinic, but they're going to charge through the roof and your insurance will definitely not cover it. Feel free to cry for pharma companies losing some fraction of their precious patent-protected dollars, but $15,000 is utterly absurd. There is no need at all to pay that much.
I don’t super want to restart the “Chinese peptide suppliers - safe or dangerous?” debate. I’ve known some people who have used them, and I don’t have any particular horror stories to share, but that just means that they won’t definitely kill you. I don’t know if the actual catastrophic failure rate is more like 1/100 or 1/1,000,000,000, and although I’m sometimes a little cavalier about pills I would be more nervous about things I inject into my body. If any of you have specific bad experiences with this kind of thing, please let me know in the comments so I can update.
3. Other Weight Loss Drugs
Karen in Montreal on why it’s hard to use stimulants for weight loss:
Doses needed for consistent weight loss/maintenance are much higher than for, say, ADHD. Plus every time the damned things wear off, ALL the hunger arrives at once. And you have to let them wear off, because otherwise sleep is terrible. (I was prescribed Dexedrine for weight loss several decades ago by a crazy doctor, and am now on a decently high dose of Vyvanse for ADHD).
I prescribe a lot of people stimulants for ADHD, and my experience is that they rarely get any useful amount of weight loss.
Arby writes:
As an interesting aside, Janssen's Invokana diabetics drug has also been proven to cause weight loss. https://www.fiercepharma.com/pharma/proof-concept-trial-j-j-s-invokana-combo-helps-non-diabetics-shed-significant-weight sadly the trials went nowhere after in 2017 invokana got slapped with a black box warning for heightened risk of big toe amputations. A risk that one may be willing to take to treat diabetes but not weight problems. There must be something in mechanism of action of diabetes drugs that causes this nice weight loss side effect.
It’s the big toe in particular surprisingly often!
I'm late commenting but I don't see anyone mentioning metformin yet.
** THIS IS NOT MEDICAL ADVICE **
Metformin is off-patent and although its only on-label use is for diabetes, some people think it extends life expectancy. (The main evidence for this is that diabetics who take metformin live longer on average than people who aren't diabetic.)
Since I started taking it my blood sugar has dropped from the high end of the normal range to the low end, which I imagine is a good place for it to be. And I've lost a noticeable thought not dramatic amount of weight: maybe 5% or thereabouts, which moved me from "overweight" to the high end of normal.
Surely people who are thinking about taking semaglutide should try metformin first?
Metformin has many good qualities and is inexpensive, but it’s probably much less effective at weight loss than semaglutide. Still, a reasonable starting point. You can find some people’s testimonials and antitestimonials in the replies to Jeff’s comment.
Ronald Eliosoff writes:
I am an internist with a longstanding interest in the medical management of obesity.
Bariatric surgery keeps getting better and better and safer and safer. A Sleeve Gastrectomy in the year 2022 is safer that a gall bladder extraction, a hysterectomy or even a TURP for benign prostate disease.
We now have strong evidence from several high quality prospective studies that obese patients who have bariatric surgery live longer and have much higher quality of lives than carefully matched patients who don’t. If I experienced biliary colic, I would not hesitate to have my gallbladder removed. If I was a woman and I had severe menorrhagia or painful periods, I would not hesitate to have a hysterectomy.
IFSO and the ASMBS, the two largest bariatric surgical associations in the world, recently updated their guideline recommendations for the first time in 30 years. They are now recommending that all patients with a BMI of 35 (except for the occasional weight lifter) should consider bariatric surgery as well as all diabetics with a BMI of 30 (about 90% of diabetics) and that surgery can even be considered in selected patients with no co-morbidities.
I completely support those recommendations. I recently posted a 17 minute highly evidence based discussion on bariatric surgery on YouTube which I think might interest you.
[…]
I am a huge fan of semaglutide and here in Canada, it is really not that expensive (about $3,000 /year).
However, for a one-shot payment of $14,000, one could get a Sleeve Gastrectomy by a world class bariatric surgeon. After that the need for meds for diabetes hypertension, arthritis, depression and heart disease all plumet!
From a societal perspective, the cost savings would be incalculable.
Ronald Eliosoff MD, FRCP
I see some bariatric surgery patients and I agree they generally do very well. The only disadvantages are: first, that surgery is scary. Second, that it’s irreversible and does leave you having a lot less appetite and ability to handle food for the rest of your life. And third, insurances only pay for it above some BMI threshold that a lot of people don’t reach (though maybe that will change if they think of it as a semaglutide alternative!). But I agree with Dr. Eliosoff that it’s very impressive.
Kevin Binz writes:
One-off GLP-1-proximal treatments may be sufficient for significant mitigation of obesity. If this bears out, would significantly alter the cost-benefit calculus.


What the heck? This is supposedly either a single dose or three doses (it’s not clear) of some new substance I’ve never heard of before, and it makes patients lose weight three times faster than constant semaglutide. If this holds up, the glorious post-obesity transhuman future will be here even faster than I thought!
4. People Challenging My Numbers And Predictions
RuralFP writes:
I think the amount of semaglutide being prescribed for weight loss is being undercounted in this post. I prescribe semaglutide regularly for weight loss but I have never once prescribed wegovy. It’s just way too hard to get approved. Instead I prescribe ozempic for impaired fasting glycemic or pre-diabetes (basically anyone with fasting blood glucose >100 or hgba1c >5.5) which seems to go through way easier. I don’t think the difference of 2mg vs 2.4mg is all that meaningful in terms of overall weight loss. Would be interesting to see what the real number is including these other diagnoses.
Thank you, I accept that this is a big reason to increase my estimate of how many people are using semaglutide for weight loss.
Leon writes:
Is it just me or is a 30% chance obesity is cut in half by 2050 really low if you expect it to be reasonably cheaper by 2040 (66% chance its less than $100/month). Do you expect there to be other factors keeping people from getting it? Doctors still insisting on diet/exercise first on a large scale? As yet unseen side effects? Something else I'm missing?
I answered that I was thinking of a combination of:
it's really hard to get half of a target group to take a drug. Do half of all hypertensive people take antihypertensives? Do half of depressed people take antidepressants? I'm not sure but I would guess no. This is by far the main reason for my skepticism.
Maybe the factors causing obesity will get worse by 2050.
Maybe these drugs won't be strong enough to get obese people all the way to normal weight.
Maybe somebody finds side effects and people stop using them.
Neo has the opposite concern:
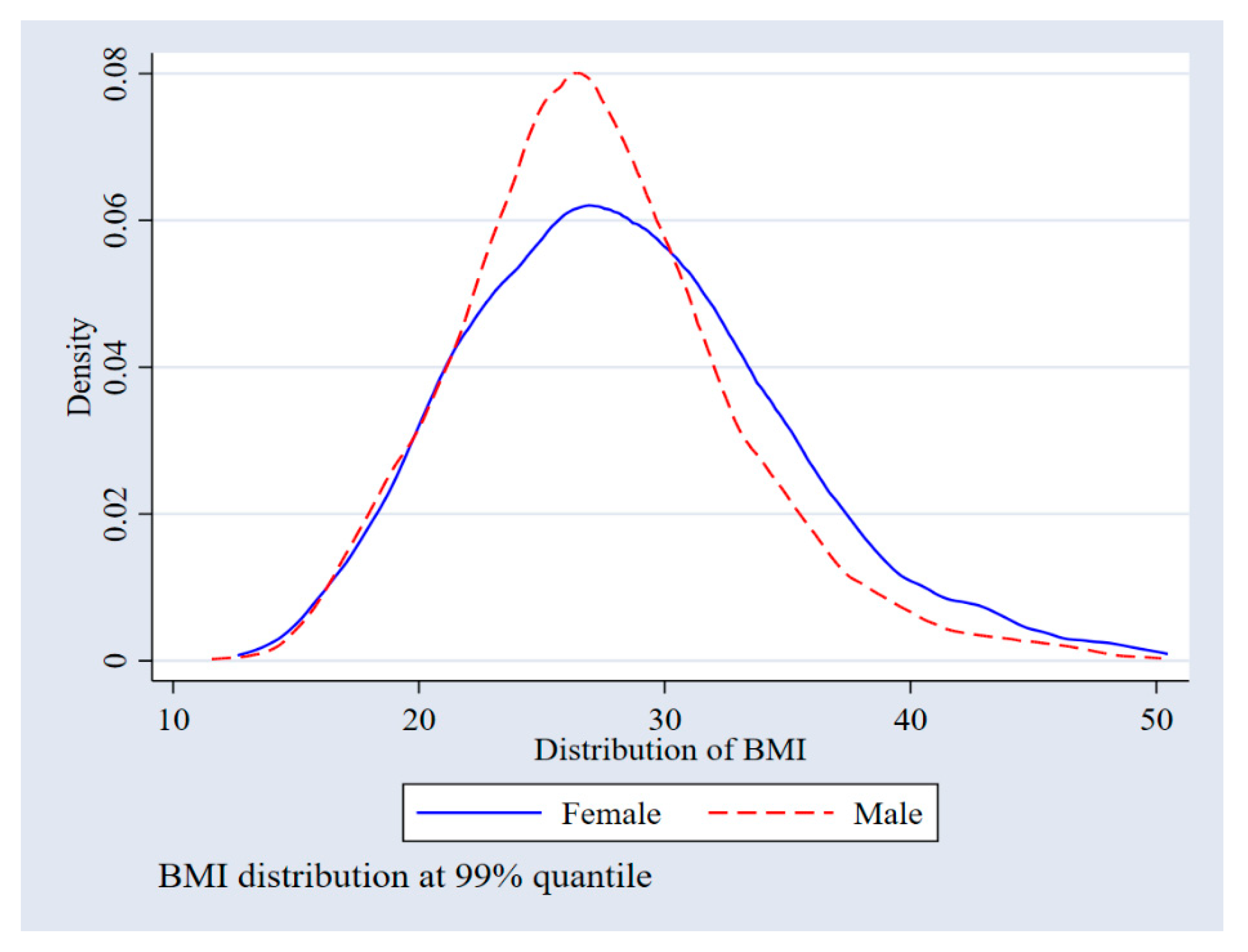
After a well reasoned article, the last line "US obesity half or less of current rate in 2050: 30%" seems to come out of nowhere. If Wegovy users on average lose only 15% of their weight, then even if 100% of obese people were using Wegovy by 2050, the obesity rate still wouldn't go down by half unless most obese people were <15% above the weight threshold that defines obesity, right?
I answered that those were good points, but:
BMI is a bell curve centered (slightly) to the left of the obesity cutoff, so most obese people will be close to the cutoff. See eg https://www.mdpi.com/ijerph/ijerph-17-02330/article_deploy/html/images/ijerph-17-02330-g001.png
Drugs might get better by 2050.
More obese people might lose more weight on semaglutide because there's more to lose (I haven't actually checked if this is true)
I think those numbers might be "over one year", and they could stay on it longer than a year.
{kind=link}
I was kind of lazy just asserting “drugs might get better”, but I think the upcoming CagriSema combination and AMG-133 are good examples of how this might play out.
Max Görlitz has done the proper thing and made Manifold markets for each of my predictions - see here, here, here, here, and here. Despite the problems with prediction markets for decades in the future, the “will obesity be cut in half by 2050” one seems popular:
5. Do You Have To Stay On Semaglutide Forever Or Else Gain The Weight Back?
Biff_Ditt writes:
I saw on the 1 year follow-up to the STEP-1 trial that most of the participants gained all of their lost weight back.
Biff is probably thinking of Weight Regain And Cardiometabolic Effects After Withdrawal Of Semaglutide, which finds people gained back 2/3 of the lost weight after a year. The graph looks like it’s in the process of plateauing but not quite there, so I don’t know if we should expect them to regain the other third later.
This matches what I would expect from my understanding of other diets and weight loss drugs. Still, some people disagree.
Maximum Liberty writes:
Anecdote is not the singular of data, but my better half lost 25 pounds on it, then had to get off it for reasons unrelated to the drug. She has not regained the weight yet -- and consistently eats less now that she had for years. So in at least one case, the drug helped with a successful change in eating habits.
Lauren Thomas writes:
So there's been a lot of research on dieting and losing weight, etc., and one of the things that has been found is that your body has a "set" point weight wise that it will try REALLY hard to return you to. If you lose weight, your body will slow its metabolism until you return to that weight. If you gain weight, your body will rev up metabolism. That's why you might gain 10 lbs over Christmas and then lose it in January without purposefully trying to lose weight. (this is all in the short term, ofc, as people do tend to naturally gain weight as they age).
This seems to imply that semaglutide would need to be taken forever. However, there seems to be an important caveat: you *can* reset your set point, it just takes a long time at the new weight. When most people go on diets and lose weight, they end up regaining the new weight quite quickly after they "end" their diet, so they don't have a chance to reset their set point.
Speaking from personal experience, I had kind of an accidental natural experiment with this: I once lost 40 lbs over the course of a year and a half, where I began with a very strict low carb diet that very very slowly trailed off to a normal diet, mostly because I got progressively more tired of being on the low carb diet. So by the time I had gotten back to my normal diet, I had been losing weight for a long time. I ended up regaining 10 lbs of the weight, but no more, and am still ~30 lbs below my peak even today (5 years later).
Something like this has been my experience with dieting too so far. And something like set point reset has to exist in order to explain things like why so many obese people fail to lose weight after they start eating healthy, and maybe other things like anorexia. And maybe it works for some people.
Still, the evidence suggests that most people who stop semaglutide will regain the weight, at least for the protocol used in the study. Maybe some other protocol that had them on it for more than a year would have done better?
6. Personal Anecdotes
Edgehopper writes:
I couldn’t get Wegovy at a reasonable price when it was approved, and then Novo Nordisk started having huge supply chain problems with their injectors. Fortunately, Eli Lilly’s coupon for Mounjaro was less restrictive at first, though they’ve had to crack down as they have trouble meeting demand for both off-label weight loss use and for the approved T2D use.
I am what the doctors call “morbidly obese,” and it’s been more effective than anything else I’ve ever tried. Down about 35 lbs in the first three months, and unlike with other diets I’ve tried, I’m not feeling miserable or hungry all the time. Assuming there aren’t scary side-effects in the future, these really are miracle drugs.
I do expect the price to come down relatively quickly due to competition, which is a good thing.
Education Realist (blog) writes:
I am on Mounjaro, and have been for four months. Lost 20 pounds so far, and I'm not yet on full dosage. Occasional mild nausea but real issue for me is....tiredness. Not fatigue or exhaustion. I'm a former insomniac who can now hit the sack at 9:00 and sleep happily to 6 am, which is insanely weird.
I have been trying to lose weight for 6 years, and for most of that time been in a 20 pound range that is 100 pounds over what someone of my height should weigh. I've eaten 1500 calories a day and not lost a pound, have to drop to 1100 to lose weight verrry slowly (that's with intermittent fasting and low carbs, around 50 grams). Last year before Mounjaro I started intermittent fasting and lost 20 pounds very quickly and then stopped cold. I do not have eating issues. I don't binge. I cut out the "four white foods" six years ago because I learned that I do better on meat and cheese and vegetables than I do on pasta or bread or potatoes and vegetables. I put on weight despite walking two and in some cases four miles a day, which I can do easily.
I am ridiculously healthy and do not have an obesity diagnosis. Stone cold normal readings in A1c, glucose, cholestrol. My doctor sent me to an endocrinologist after I lost 20 pounds and then stopped cold despite the same behavior (which I still do today) because she agreed I might be insulin resistant. Endocrinologist shrugged, said it's multifactorial, but agreed that anyone with my numbers, appearance, and obvious good health was clearly doing everything right and put me on Mounjaro with no further questions. Diagnosis: insulin resistance. My insurance pays around $500 but I'm on the $25 coupon.
I didn't change a single thing about my eating habits and lost ten pounds in 2 months on the low dosage. Higher dosages have finally reduced my appetite somewhat, but my endocrinologist and I have decided to stop the increases at 12.5 (15 is the top) and then maybe even reduce, since my appetite is decreasing but the weight loss rate is constant.
Because I lost weight doing the same behavior and no drop, I'm quite convinced that something far different than appetite suppressing is also going on (fwiw, I was on phentarmine back in the day and liked it fine). Mounjaro is supposed to increase insulin production and reduce the liver's sugar production, although what that means I dunno.
I have no idea what's up with obesity but the idea that it's all about cutting intake and exercise is just stupid. I should have been losing weight for all of the past six years and haven't. Plenty of people eat healthily and are still obese. We're probably the descendants of famine survivors.
Anyway, I wrote about it here: https://educationrealist.wordpress.com/2022/10/09/weight-loss-and-mounjaro
Eliezer Yudkowsky writes:
I tried semaglutide and it did nothing to slow rate of weight gain, just produced stomach upset, going up to 2.4mg injectable. I know one other person trying semaglutide and they reported something similar. I wonder if they played some clever games with their choice of patients. My expectation of how the news goes here is a whole lot of people who try semaglutide, maybe after fighting really hard to get on it, and find that it does nothing. That said, I know at least one friend of a friend, if not a friend per se, who claims that semaglutide was their miracle drug. So maybe still worth that hard fight, even if I'm guessing that the real proportion who get nothing out of it will prove to be over 50% in real populations.
Further fun fact: Semaglutide comes heavily recommended with diet and exercise and many stern injunctions about that! The actual insert sheet includes a graph for how much weight people lose with and without "lifestyle interventions" added. The two graphs are roughly the same.
Lan writes:
I wonder about the adoption of the medication, though. I took victoza (=saxenda, but approved for diabetes) and the absence of the desire to eat lead to some unforeseen lifestyle side effects. Given that 5 almonds made me full for the day, I was not interested in having dinner with the family or going out with friends. There is the reality that some restaurants would probably not be happy if you only ordered the smallest appetizer. In addition, alcohol was also very difficult, because the drug slows down gastric emptying and your stomach ends up absorbing alcohol for hours. I got really, really drunk for an entire night from a single glass of wine once.
Before taking this drug I had not fully appreciated how much of one's (social) life revolves around food; lunch break with colleagues, dinner with family or friends, drinks on the weekend, a sweet treat, snacks and a movie etc. But once I was not interested in food anymore, combined with the tiredness that comes with eating little, a lot of those activities also lost their appeal. (On the upside, I slept like a log.)
Walter Sobchak, Esq writes:
I have been taking Wegovy for 14 months. When I began I weighed 275 lbs and my BMI was 39.9. I have hypertension, albeit well controlled by medicines. Diet and exercise phaaahhh. I could eat faster than I could exercise. And no, I eat very little fast food and little candy and soda.
I worked with my doctor to be prescribed Wegovy. It was only approved by the FDA in June 2021. My doctor was reluctant because he was unfamiliar with the class of compounds. He does not like to prescribe off label so he was not willing to to start me on Ozempic. But, the FDA solved that problem.
I knew to ask for the drug because my daughter was pre-diabetic and had been put on Metformin and Ozempic. She lost 100 lbs. in 2019 and 2020.
I started on Wegovy in September 2021. I now weigh 220 and my BMI is 31.5. That represents a 20% reduction in my original weight. 220 was my original goal. To get a BMI under 30 I would have to be under 209. I doubt that I will get there. I am back in 40 in. trousers which I had not been able to wear in 30 years. 220 was my original goal.
I have had no major side effects other than constipation. Even that is a little hard to tease out. I am on 7 Rx drugs and at least 5 of them are constipating. I have been pounding Metamucil and Colace for years.
I have been able to fill my prescriptions using a GoodRx coupon at $1328 for a box with 4 injectors. A year requires 13 boxes. The total cost for 15 boxes has been about $20,000.
I can afford it and it has been worth while. I call it a bargain, the best I've ever had.
I understand that it still way too expensive for the American health care system to afford. But given the bonanza size of the market. There will be lots of competition starting with the Lilly's tirzepatide. There are several other pharma's with GLP-1 agonists in development. I am sure that the cost will come down.
My doctor tells me that I can expect to stay on semaglutide for the long term. He is proposing that I switch to Ozempic 2 mg for maintenance as I can buy that for less than $1,000 for a four dose pen.
My only sadness is that semaglutide wasn't invented 40 years ago when i would have saved me from a lot of damage. But, I am grateful that it exists now and that it has helped my daughter so much.
Also from Walter, and I was wondering about this:
I was very concerned with the injections before I started Wegovy. My experience is that the injector is fast and almost painless. My pharmacist was important because he showed me how to do it correctly before I started.
7. Tangents That I Find Tedious, But Other People Apparently Really Want To Debate
Why can’t people just diet and exercise? (142 comments)
Why can’t people just go to the gym? (72 comments)
Does our society overprescribe pills as quick fixes? (99 comments)
What about the SMTM potato-only diet? (13 comments)
Is BMI a good measure of obesity? (8 comments)
Share this post